Risk of Ovarian Malignancy Algorithm: ROMA®
ROMA
ROMA, the combination of CA125 + HE4 tests, along with menopausal status, is used to help determine the likelihood of finding a malignancy on surgery in women who present with adnexal mass. Risk stratification helps ensure optimal patient care by promoting the triage of patients at high likelihood of ovarian malignancy to tertiary care centers with multidisciplinary teams that specialize in ovarian cancer.
During a study, ROMA was evaluated in 472 women with adnexal mass who were initially assessed by generalist Ob/Gyns and primary care physicians and subsequently underwent surgery. ROMA correctly identified 94% of women with an epithelial ovarian cancer as high likelihood of malignancy. These patients can be referred to specialized gynecologic oncologists for optimal care. At the same time, 75% of patients with benign disease were correctly identified and could undergo treatment by their gynecologist in the community.2
ACOG & ROMA Score
ACOG recommends ROMA as one of the several risk assessment algorithms when referring patients with an adnexal mass.5
ACOG Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses November 2016
- CA 125 level is elevated in only one half of cases of early stage epithelial ovarian cancer and rarely in cases of germ cell, stromal, or mucinous cancer
- Serum biomarker panels may be used as an alternative to CA 125 level alone in determining the need for referral to or consultation with a gynecologic oncologist when an adnexal mass requires surgery.

Summary
The combination of CA125 + HE4 accurately determines likelihood of malignancy:2
-
Many markers have been studied, but the CA125 + HE4 combination has proven to be a more accurate predictor of malignant disease than either marker alone.1
-
Patients classified as being at increased likelihood of malignancy for ovarian cancer can be referred to a gynecologic oncologist (GYN/ONC) for optimal care.3,4
-
In a prospective multi-center study, the combination assay yielded a sensitivity of 94%, with a fixed specificity of 75%.2
Watch the Full 5-Minute Video -
This evidence-based 5-min educational video provides guidance on the adjunctive use of the ROMA® Score to reduce false negatives when evaluating patients with an adnexal mass.
1.Understanding the Clinical Utility of ROMA in the Evaluation of Women with an Adnexal Mass
Clinical Education Video (5:08)

Clinical Education Miniseries - Evaluation of an Adnexal Mass
Part 1: The Importance of Proper Referral of an Adnexal Mass
Clinical Education Video Mini-Series - The Importance of Proper Referral of an Adnexal Mass (1:03)
Part 2: Limitations of CA 125 in Adnexal Mass Risk Assessment
Clinical Education Video Mini-Series - Limitations of CA125 in Adnexal Mass Risk Assessment (:45)
Part 3: The ROMA Score and Clinical Utility
Clinical Education Video Mini-Series - The ROMA Score and Clinical Utility in Adnexal Mass Risk Assessment (:55)
Part 4: Clinical Case Examples Using the ROMA Score
Clinical Education Video Mini-Series - Clinical Case Examples of Using the ROMA Score (1:30)

Part 5: Ordering the ROMA Score
Clinical Education Video Mini-Series - Ordering the ROMA Score (:35)
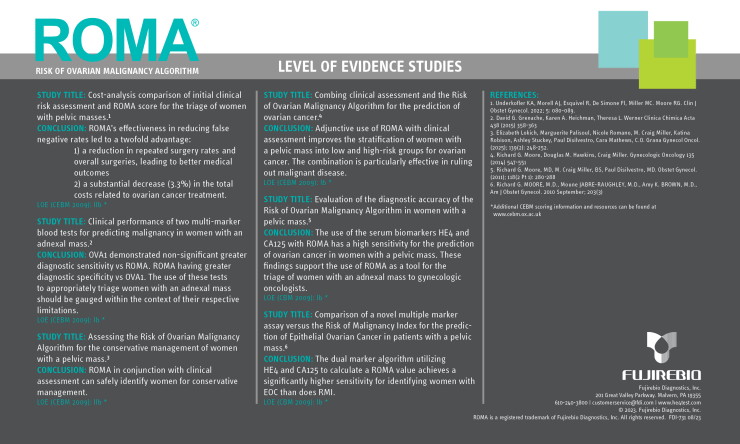
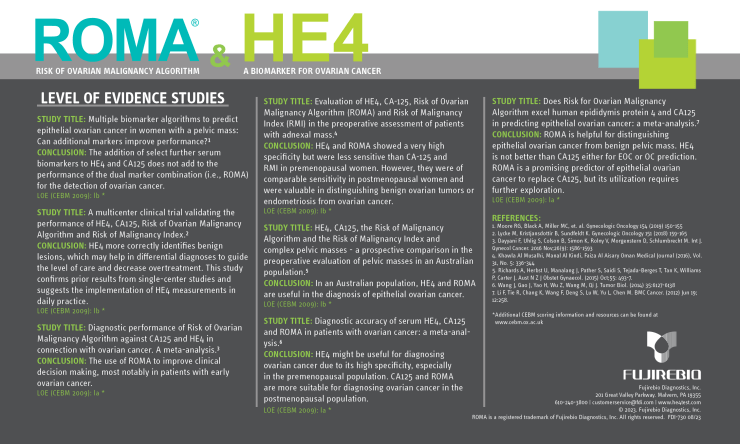
Level of Evidence
The level of evidence (LOE), also known as a hierarchy of evidence, highlights the most relevant and updated scientific research in the field and can be considered the strongest form of evidence. Levels of evidence are assigned to studies based on the research design, quality of the study, and applicability to patient care. According to the Oxford Centre for Evidence-Based Medicine, there are five levels in this hierarchy of evidence: Level 1 represents strong, high-quality evidence, while Level 5 indicates evidence with effectiveness not established.6 Higher-quality evidence (Level 1) has less risk of bias. Please download and review Fujirebio's public level of evidence studies below.
ROMA Intended Use
The Risk of Ovarian Malignancy Algorithm (ROMA®) is a qualitative serum test that combines the results of HE4, CA125 and menopausal status into a numerical score. ROMA is intended to aid in assessing whether a premenopausal or postmenopausal woman who presents with an ovarian adnexal mass is at high or low likelihood of finding malignancy on surgery. ROMA is indicated for women who meet the following criteria: over age 18; ovarian adnexal mass present for which surgery is planned, and not yet referred to an oncologist. ROMA must be interpreted in conjunction with an independent clinical and radiological assessment. The test is not intended as a screening or stand-alone diagnostic assay.
PRECAUTION: ROMA should not be used without an independent clinical/radiological evaluation and is not intended to be a screening test or to determine whether a patient should proceed to surgery. Incorrect use of ROMA carries the risk of unnecessary testing, surgery, and/or delayed diagnosis.

References
- Moore RG, Brown AK, Miller CM, et al. The use of multiple novel serum tumor markers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol Oncol. 2008;108(2):402-408.
- Moore, R.G., et al., Evaluation of the diagnostic accuracy of the risk of ovarian malignancy algorithm in women with a pelvic mass. Obstet Gynecol, 2011. 118(2 Pt 1): p. 280-8.
- Guidelines for referral to a gynecologic oncologist: rationale and benefits. The Society of Gynecologic Oncologists. Gynecol Oncol. 2000;78(3 Pt 2):S1-S13.
- Giede, K.C., et al., Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol Oncol, 2005. 99(2): p. 447-61.
- ACOG Practice Bulletin No. 174. Obstet Gynecol 2016;128:e210–26
- OCEBM Levels of Evidence — Centre for Evidence-Based Medicine (CEBM), University of Oxford